 Ελληνικά
Ελληνικά English
English
Scientific Support »
The staff of the teams has to screen the players, identify any possible injurie risks and weaknesses and put in place individual trainings to help reduce the occurence of them as also to the safe return from an injury incident.
The staff of the teams has to screen the players, identify any possible injurie risks and weaknesses and put in place individual trainings to help reduce the occurence of them as also to the safe return from an injury incident.






The hip rotators are mostly located at the posterior aspect of the hip (Table 1). The hip external rotators specifically are considered important for the execution of the instep and side-foot kicks (1, 2). It has been theorized that excess stress stemming from the execution of repetitive movements may result in muscle tightness (3). Given that instep and side-foot kick are fundamental activities in soccer practice, it may be concluded that these muscle groups may be susceptible to tightness. A less than optimal range of motion may affect quality of force production and application and will be associated with energy leaks (4). In addition poorly conditioned hip rotators may lead to abnormal lumbo-pelvic posture and lumbar spine motion during athletic movements (5).
|
External rotators |
Internal rotators |
|
Psoas |
Gluteus medius (anterior fibers) |
|
Illiacus |
Gluteus minimus |
|
Sartorius |
Adductor magnus (anterior fibers) |
|
Gluteus maximus |
Adductor longus |
|
Gluteus medius (posterior fibers) |
Adductor brevis |
|
Biceps femoris (long head) |
TFL |
|
Adductor magnus (posterior fibers) |
ST/SM |
|
Piriformis |
Table 1. External and internal rotators of the hip joint.
Research indicates that the hips are affected in soccer players since hip-rotation ROM decreases over the years in soccer players (6) and both youth and senior footballers have significantly less internal rotation (and significantly higher abduction) than their respective age-matched controls (7). In addition higher decrease in hip range of motion (possibly due to internal rotation lessening) that is strongly associated with ACL ruptures has been reported in soccer players when compared with the general population (8), whilst soccer players with re-rupture of the ACL have significantly lower mean internal-external hip rotation when compared with healthy professional soccer players (9).
Tightness within the hip external rotators will limit hip internal rotation and tightness within the hip internal rotators will limit hip external rotation (3, 4). Given that all muscles listed in Table 1 are also implicated in the execution of other hip movements, profiles of hip extension/flexion and abduction/adduction along with external/internal rotation may provide to the strength and conditioning professional a starting point for interventions on an individual basis.
REFERENCES
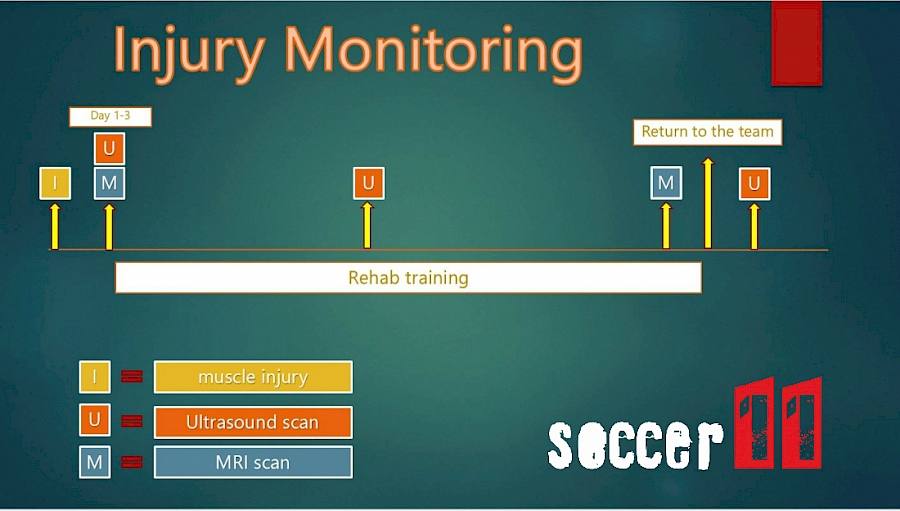
The most appropriate way to monitor the reintegration of a player in a team training process is the sequential execution of ultrasound and MRI as in Figure 1. In this way the medical staff and the fitness coach of the team work methodically and with safety protection with regard to athlete's rehabilitation program in a healthy condition and in full readiness.
Hip flexion plays a vital role in many athletic as well as every day life movements (1). Flexion at the hip involves the action of many different muscles (Figure 1).

The muscles responsible for hip flexion are:
In most cases the term “hip flexors” is quite generic or even vague due to the plethora of muscles with different lever arms and therefore different potential for force production at different degrees of hip flexion (2). The study of anatomical leverages of the above muscles has been the central point of our understanding regarding their function during hip flexion. The psoas and the iliacus are the only muscles of the hip flexor group that their insertion is inferior to the pelvis (2, 3). More specifically the psoas has its origin from the length of the lumbar spine, while the iliacus originates on the posterior of the ilium (3). Therefore the psoas and the iliacus are the only muscles with a lever arm above 90º of hip flexion (2, 3). It has been proposed that in the case of a weak psoas or iliacus, the femur may move above the level of the hip, but it is not from the action of these muscles, but rather from the momentum created by the other hip flexors; that is the psoas and the iliacus are the only hip flexors capable of actively bringing the hip above 90º (4, 5).
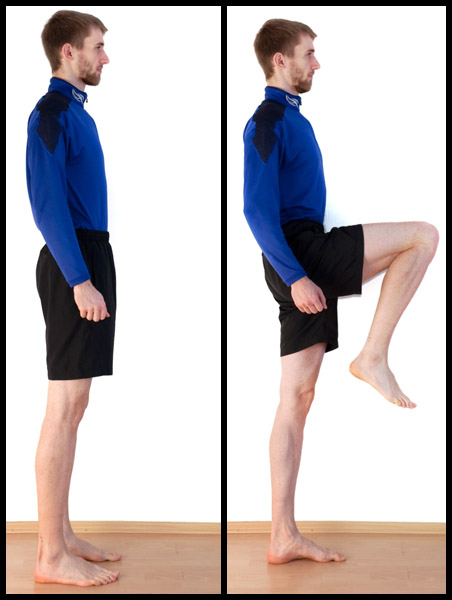
A simple test to assess the function of the psoas and iliacus is to pull one knee to the chest and release while in a single-leg stance (2). Inability to keep the knee above 90º for 10-15 seconds indicates a weak psoas/illiacus or both (2, 5).
A more advanced test especially for athletic population would be to have your athlete stand with one foot on a plyo box so as the knee is set at above hip height (for most average height athletes this would mean a 60cm plyo box) (4). The athlete places his hands overhead or behind the head and attempt to lift the foot off the box and hold it up for 5 seconds. Inability to lift and hold is indicative of a weak psoas or iliacus, or both (4).

REFERENCES
Meniscal injury ruptures are frequent injuries in the football field. The heavy loads and the direct percussions the knee receives during training and matches increase the chances of this particular injury occurring. The following program is indicative and refers to the final stage of rehabilitation after arthroscopic surgery and if the athlete has undergone the required stages of treatment and strengthening.

-Start your athlete with a warm up on a static bike combination with static / dynamic stretches to increase knee joint mobility and muscle elasticity.
-Continue with preactivation exercises to prepare the muscles.
-Perform propioception exercises to activate the C.N.S and the propioceptors.
- Allow the player to perform the first stage of warm-up (low-intensity) with the team (for psychological reasons too).
- Improve the player's endurance capacity with interval training on his maximum aerobic speed
2 x 6' with 2' stop (10 '' strong run -20'' drive the ball-10'' strong run-20 '' static juggle with a ball)

-At the end of the endurance program or at another time of the day (preferable) follow a strength training program with the 5 exercises of the picture
- Finish the program with static stretching and Foam Roler .

